My research is fundamentally concerned with improving the lives of those affected by communication impairment. Informed by my clinical experience, I pursue this by better accounting for the individual, by architecting predictive models that facilitate clinical decision-making about how and when to intervene, and by designing assessments that treat communication, the damaged brain, and its surrounding contexts more holistically.
Specific questions include, but are not exclusive to: Who will recover with standard care, and who will not, early enough for the answer to guide treatment? What do standardized assessments overlook when they collapse performance into a single score? Once a patient is unlikely to improve on their own, which treatment, at what dose, and for whom, will alter the course? I am also thinking about what data and models can and cannot reliably tell us about these conditions and their trajectories, and why; how to make our approaches more interdisciplinary; and how to better characterize populations historically neglected in research on stroke and language, e.g., profoundly impaired individuals, multilingual speakers, and patients whose damage is not confined to the left hemisphere.
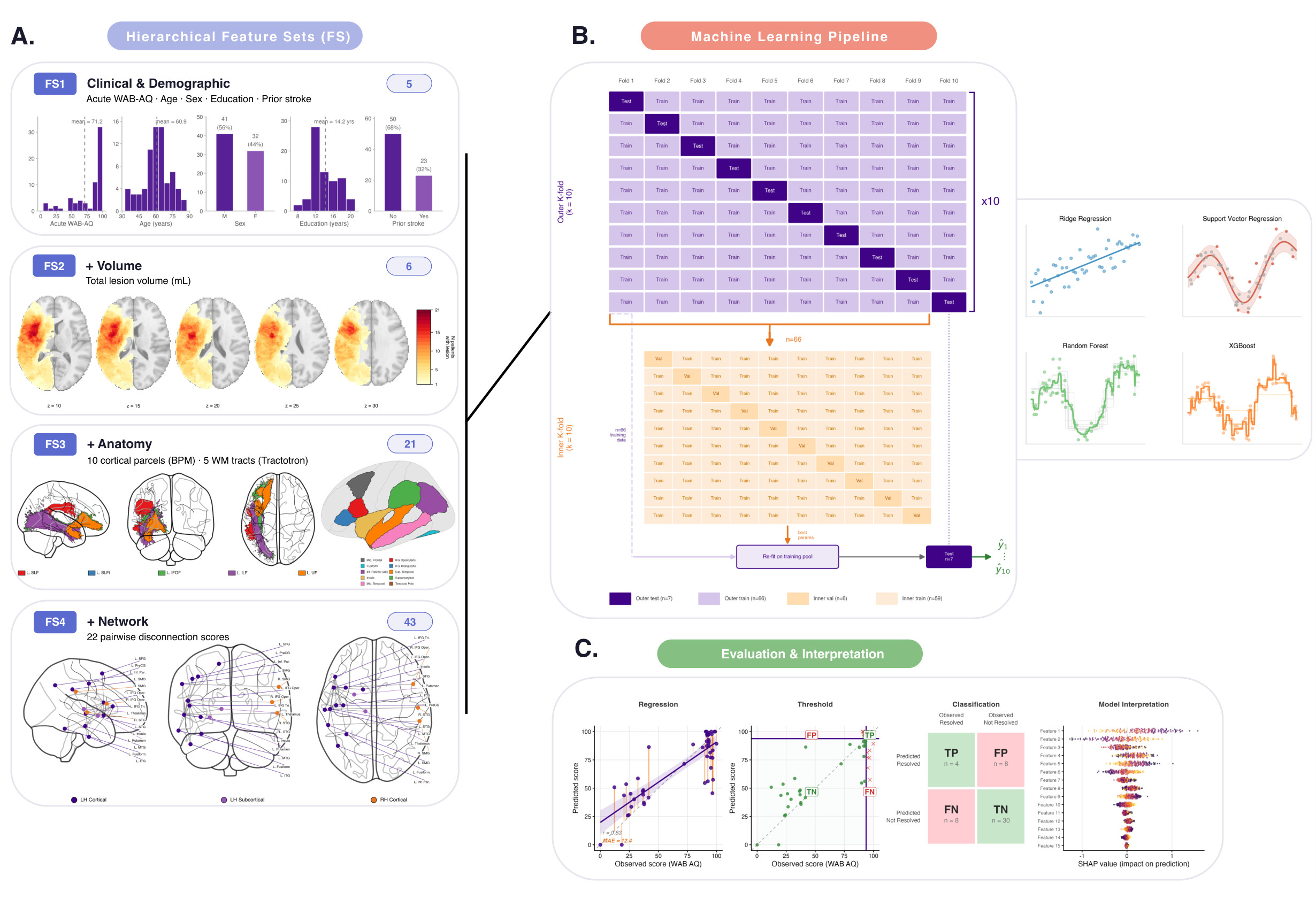
Computational prediction of recovery
I build machine learning models that integrate behavioral, demographic, and structural-imaging features to forecast the magnitude, language, and time course of aphasia recovery, from acute prognosis within days of stroke to treatment response in the chronic phase.
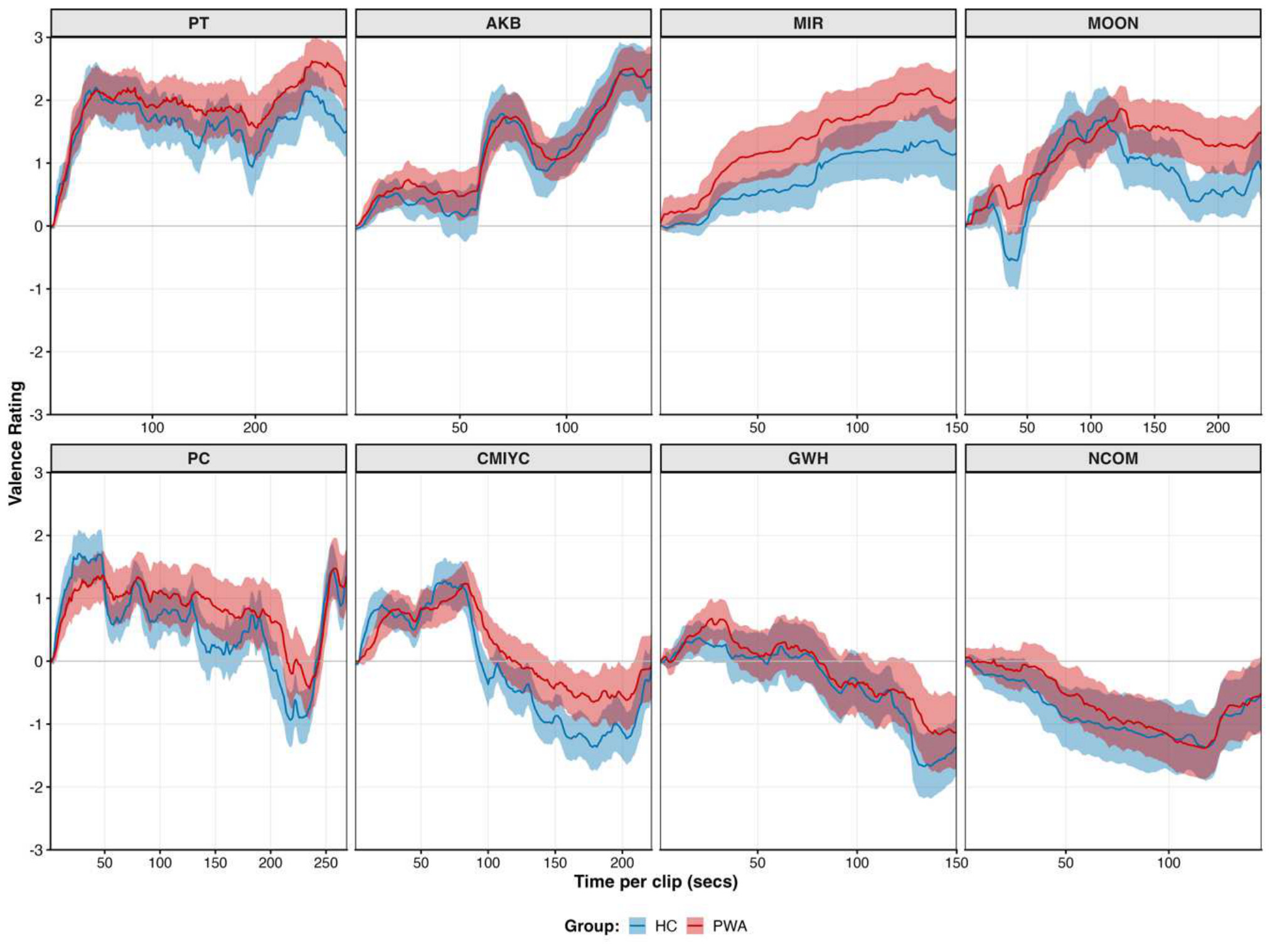
Measurement beyond standardized assessment
Standardized batteries reduce language to a single severity dimension; I develop discourse-based and naturalistic, multimodal measures, e.g., connected-speech analysis, continuous affect rating and eye-tracking during movie-viewing, and LLM-augmented main-concept scoring, that index the linguistic, emotional, and attentional processes such testing renders invisible and that expose residual deficits in patients standard criteria classify as recovered.
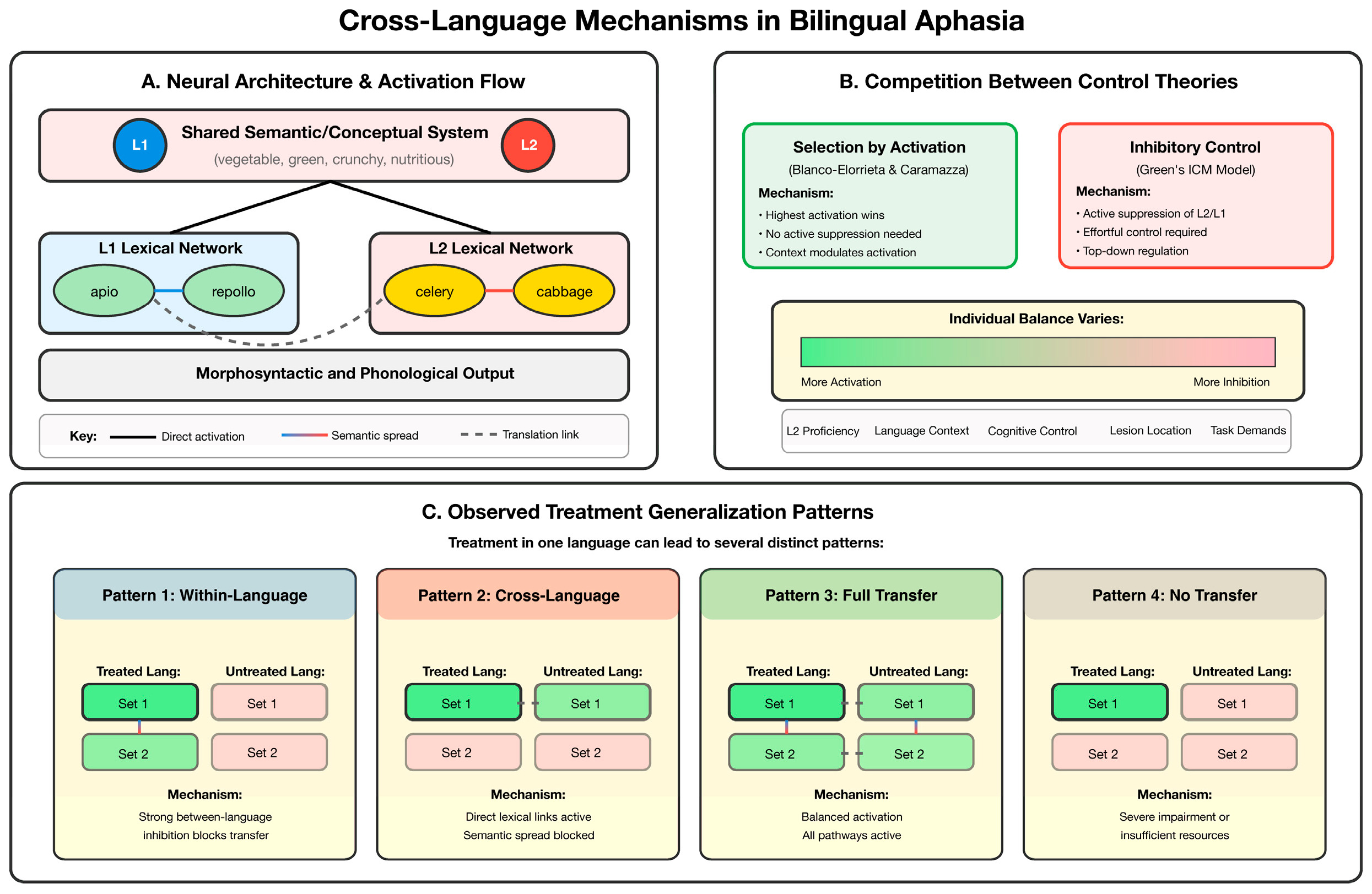
Bilingual and multilingual aphasia
In bilingual and multilingual aphasia, I study how recovery can be better predicted and supported by accounting for patient-specific factors. How do bilingual language experience and demographic factors shape treatment response and cross-language generalization? How can linguistic structure such as cognate overlap be exploited to refine clinical assessment? And do a speaker's two languages draw on a single, integrated lexical-semantic system?